Many behavioral health practices believe revenue issues begin when a claim is denied. In reality, the problem usually starts much earlier, often at intake, documentation, or authorization. This is where behavioral health revenue cycle management plays its most important role.
Revenue cycle management (RCM) isn’t just about billing and collections. It’s the full process of how a clinic captures, manages, and secures revenue from the moment a patient schedules an appointment to the final payment posting. When any part of that cycle breaks down, the financial impact can quietly grow over time.
Behavioral health practices face unique challenges that make RCM more complex than in many other medical specialties. Understanding how the revenue cycle works and where it commonly fails can help clinics reduce denials, stabilize cash flow, and spend less time reacting to billing problems.
What Revenue Cycle Management Means in Behavioral Health
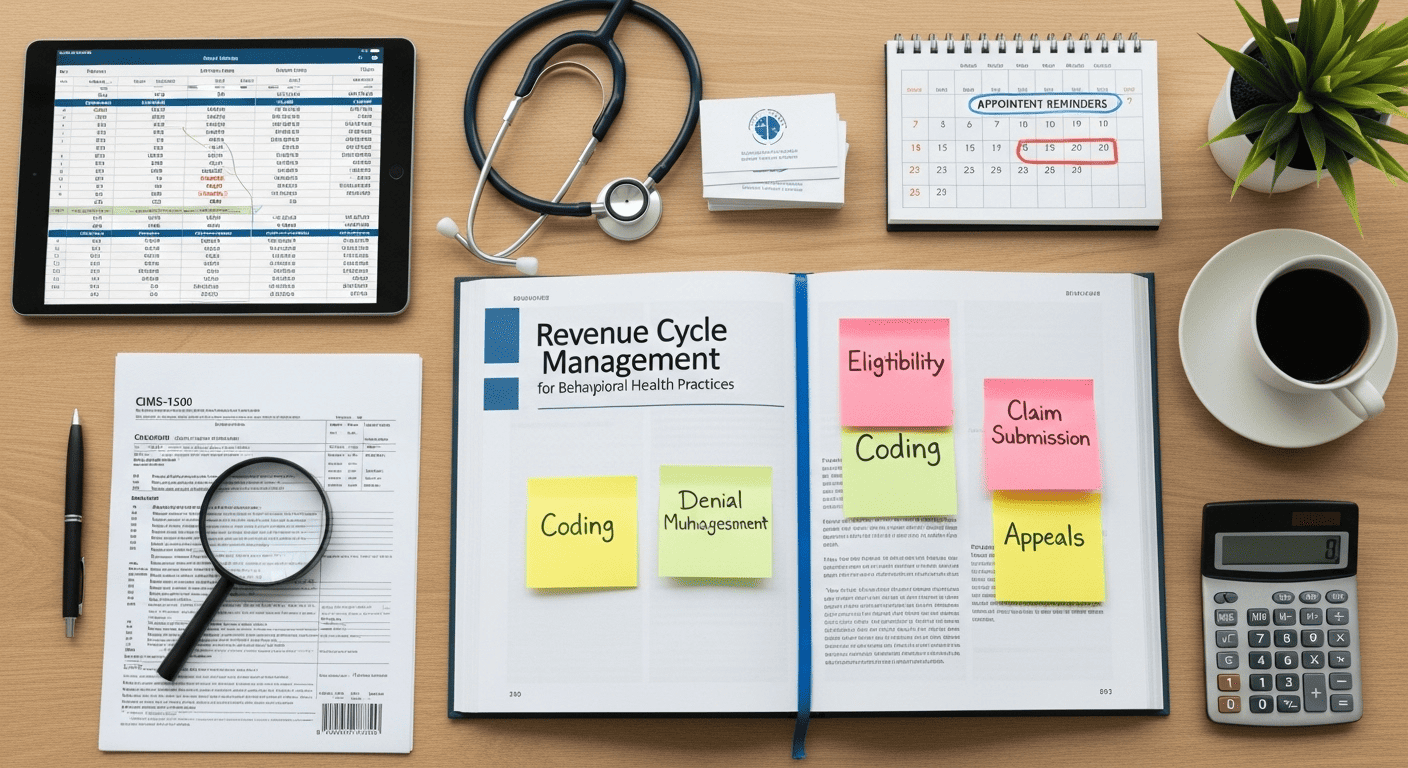
At its core, revenue cycle management refers to the systems and workflows used to track patient care episodes from eligibility verification through reimbursement.
In behavioral health, the behavioral health revenue cycle includes several additional layers of complexity:
- Authorization requirements tied to medical necessity
- Time-based and session-based billing
- Frequent documentation reviews by payers
- Diagnosis-driven coverage limitations
- Multiple levels of care, including Outpatient, Intensive Outpatient Programs (IOP), Partial Hospitalization Programs (PHP), Residential Treatment, and Detox services
Because of this, RCM for behavioral health practices requires more coordination between clinical, administrative, and billing teams than many providers expect.
The Key Stages of Behavioral Health Revenue Cycle Management
Understanding the revenue cycle is easier when it’s broken into clear stages. Each stage builds on the one before it, and mistakes early in the process often surface later as denials or delayed payments.
Patient Intake and Insurance Verification
Everything starts at intake. Accurate patient information, insurance verification, and benefit confirmation set the foundation for the entire billing process.
Common challenges at this stage include:
- Incomplete insurance verification
- Misunderstanding behavioral health coverage limits
- Not identifying authorization requirements early
- Errors in demographic or policy details
When verification is rushed or treated as a formality, the downstream effects can be costly.
Authorizations and Medical Necessity
Behavioral health services are frequently subject to prior authorization. These approvals are often diagnosis-specific, time-limited, and tied to clinical documentation.
Issues arise when:
- Services exceed authorized dates or units
- Levels of care, such as including Outpatient, Intensive Outpatient Programs (IOP), Partial Hospitalization Programs( PHP), Residential, or Detox, change without updated approval
- Documentation doesn’t clearly support ongoing treatment
Authorization tracking is a critical but often underestimated part of revenue cycle management behavioral health workflows.
Clinical Documentation
Documentation is the bridge between care delivery and reimbursement. In behavioral health, payers closely review notes to confirm medical necessity and service accuracy.
Problems occur when:
- Progress notes don’t align with billed services
- Treatment plans lack measurable goals
- Diagnoses aren’t clearly linked to interventions
- Required credentials or signatures are missing
Even clinically sound care can go unpaid if documentation doesn’t meet payer standards.
Coding and Charge Entry
Coding translates clinical care into billable claims. Behavioral health coding requires careful attention to session length, provider credentials, and CPT code rules.
Common errors include:
- Billing incorrect time thresholds
- Using outdated codes
- Mismatching services and diagnoses
- Incorrect modifiers
These medical billing errors in behavioral health are a major source of avoidable denials.
Claims Submission and Payer Review
Once claims are submitted, payers review them for accuracy, coverage, and compliance. Behavioral health claims often face more scrutiny due to medical necessity guidelines.
Delays or denials may stem from:
- Missing information
- Inconsistent documentation
- Authorization mismatches
- Payer-specific policy rules
This stage often reveals issues that originated much earlier in the revenue cycle.
Payment Posting and Reconciliation
Accurate payment posting ensures that reimbursements match payer contracts and billed amounts.
Challenges include:
- Partial payments that go unnoticed
- Incorrect adjustments
- Secondary insurance coordination issues
- Lack of clarity on patient responsibility
Without careful reconciliation, clinics may never realize they were underpaid.
Denial Management and Follow-Up
Denials are inevitable, but unmanaged denials become permanent losses.
Effective denial management involves:
- Identifying denial trends
- Correcting root causes
- Submitting timely appeals
- Tracking outcomes
Many practices struggle here due to limited staff time or unclear workflows.
Insurance-Specific Expertise Matters
Many behavioral health revenue issues arise because each payer follows different rules for authorization, documentation, and reimbursement.
This revenue cycle management approach is specialized for behavioral health providers working with BCBS, Tricare, and Medicaid. Understanding payer-specific expectations helps reduce denials, prevent delays, and improve approval rates.
Specialized support is especially important for managing IOP, PHP, Residential, and Detox services, where medical necessity reviews and authorization limits are strict and frequently monitored.
Common RCM Mistakes Behavioral Health Practices Make
Treating RCM as “Just Billing”
One of the most common misunderstandings is viewing RCM as a back-office function rather than a full operational process. When intake, clinical teams, and billing operate in silos, errors multiply.
Relying on General Medical Billing Knowledge
Behavioral health billing has its own rules. Practices that rely on general billing approaches often see higher denial rates because payer expectations differ significantly.
Inconsistent Documentation Standards
When clinicians document differently or aren’t trained on payer expectations, claims become harder to defend.
Weak Denial Tracking
Denials aren’t just individual problems; they’re data points. Without tracking patterns, clinics miss opportunities to fix systemic issues.
Practical Ways to Strengthen Revenue Cycle Management
Improving RCM doesn’t require perfection; it requires structure and awareness.
Standardize Intake and Verification Processes
Clear checklists and verification protocols reduce preventable errors.
Align Clinical and Billing Teams
Open communication helps ensure documentation supports billing requirements.
Monitor Authorization Timelines
Tracking approvals prevents accidental overuse or expired services.
Review Denials Regularly
Patterns reveal where processes need improvement.
Consider Specialized Support
Many clinics partner with billing services for mental health providers to gain expertise without expanding internal staff.
An Expert Perspective: Why Experience Matters in Behavioral Health RCM
Revenue cycle management in behavioral health is both technical and interpretive. It requires understanding payer behavior, anticipating documentation questions, and knowing how to respond when issues arise.
Experienced RCM professionals don’t just react to denials; they work upstream to prevent them. That perspective often comes from hands-on exposure to payer audits, appeals, and evolving coverage rules.
For many practices, this is where specialized RCM for behavioral health practices adds value not as a replacement for internal teams, but as structured support.
Conclusion:
Revenue challenges in behavioral health rarely come from a single mistake. They grow from small breakdowns across the revenue cycle.
With increasing complexity around IOP, PHP, Residential, and Detox billing, especially for BCBS, Tricare, and Medicaid, proactive revenue cycle management is essential.
By understanding how behavioral health revenue cycle management works and where it commonly fails, practices across Massachusetts can take proactive steps to protect revenue, reduce stress, and focus more fully on patient care.
FAQs
- What makes revenue cycle management different in behavioral health?
Behavioral health involves stricter authorization rules, documentation requirements, and payer reviews compared to many medical specialties. - Why do behavioral health claims get denied so often?
Denials usually stem from documentation gaps, authorization issues, or coding errors earlier in the revenue cycle. - Is RCM only about billing and collections?
No. RCM includes intake, verification, documentation, coding, claims, payments, and denial management. - Can small RCM issues really affect cash flow?
Yes. Small issues repeated over time often result in significant revenue loss. - When should a practice consider outside RCM support?
When denials persist, payments are delayed, or internal staff struggle to keep up with payer requirements.